
The US is fighting a modern pandemic with a 1990s-sized workforce.
As a fourth-year medical student, Adrienne Green recently found herself facing what she says her peers might call “a nuclear-level disaster.”
Green is an aspiring vascular surgeon who expects to graduate from Loma Linda University’s medical school in California this May. For most students like her, graduation isn’t the end — it’s really just the beginning. After medical school, newly minted physicians usually join hospital-based residency programs, where they complete anywhere between three to nine years of on-the-job training before becoming fully licensed independent practitioners.
The problem facing Green was that the computer algorithm intended to pair her with a residency program had left her empty-handed: Like more than 2,000 of her graduating peers across the country, she hadn’t matched, leaving her — at least temporarily — without a clear path to becoming a surgeon. “To get through the pipeline, and not find a job, is a bit jarring,” she said.
Residency training is the fire that forges medical school graduates into independently practicing doctors, which the US desperately needs more of. According to the Association of American Medical Colleges (AAMC), the country is currently short about 20,000 physicians, and the gap is estimated to rise to between 38,000 and 125,000 by 2034, depending on demographic shifts, economic uncertainties, and changes in health care use.
The American physician shortage existed well before Covid-19. But the shortage both stymied the US response to the pandemic and grew more severe than experts predicted due to pandemic-related burnout and accelerated retirement.
But despite the great need for more doctors, there are still huge gaps between the number of aspiring physicians and the space available to train them, a dynamic that keeps perfectly well-qualified medical school applicants and graduates out of the pipeline.
In 2021, for instance, there were a record-setting 42,508 active applicants for residency programs — 3,741 more than in 2020 — but only 35,194 first-year positions, according to the National Resident Matching Program. Although the number of residency spots has been creeping upward in recent years, the growth has not been fast enough to close the gap.
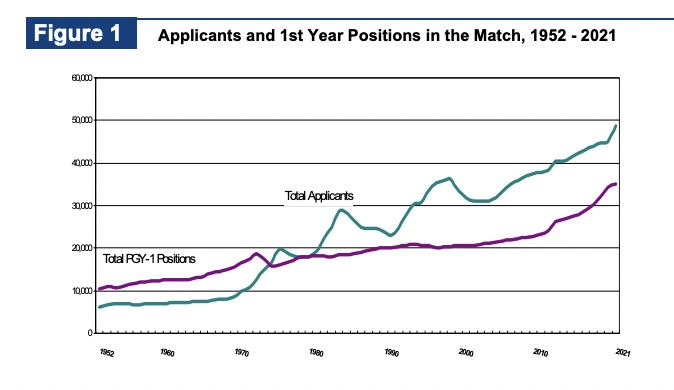
National Resident Matching Program
At the root of the mismatch between physician supply and demand are decades-old limits on medical school enrollment and outdated rules governing the federal funding for most residency programs. While Congress has taken some baby steps toward increasing that funding, it has yet to make the kinds of bold changes necessary to create a sustainable and pandemic-resilient physician workforce.
The US doctor shortage is bad, and it’s about to get worse
The US medical system falls behind those of our peer countries in so many ways. We have higher administrative costs and worse outcomes than other high-income countries — and we also have fewer physicians available per person.
“If you take a look at EU countries that have sophisticated medical systems,” explained Janis Orlowski, chief health care officer at the AAMC, “they have between 30 and 40 physicians per 10,000 people. In the United States, we have about 26 to 27.”
It’s not an apples-to-apples comparison, in part because physicians use their time differently in different systems. But it’s clear the shortage is a burden, and it’s likely to get worse as the US population grows larger and older.
According to a report published last June by the AAMC, the current US population of about 330 million will likely balloon to 363 million by 2034. By then, the number of Americans 75 and older will increase by a whopping 74 percent compared to 2019 numbers. This portends a big uptick in the need for physicians because older people generally use more medical services.
As demand for medical practitioners grows, more and more physicians will also leave the profession entirely. In a December 2021 survey conducted by the American Medical Association, one in five physicians said they would likely leave their current practice within two years, and about a third said they’d likely reduce their work hours in the next year.
The larger workforce trend has been dubbed the “Great Resignation,” and the reasons doctors are quitting echo the factors contributing to shortfalls among other health professionals, including nurses, medical assistants, physical therapists, and pharmacists. Burnout, fear of exposure, pandemic-related mood changes, and workload were all associated with intent to leave the profession.
An intensified physician shortage would be bad for the nation’s health. Life expectancy is lower — and mortality due to cancers and heart and lung disease is higher — in areas with fewer primary care providers, and those with fewer OB/GYNs have higher maternal and infant mortality rates. And in states with large populations outside big cities, rural physician shortages are linked with a variety of negative health outcomes.
Orlowski said that to avert the projected physician shortage, the number of new resident positions available annually would have to double to a total of 70,000 nationwide for the next two to three years, then stay at a rate of around 40,000 new residents a year for the foreseeable future.
For a variety of reasons, that’s a wildly unrealistic scenario. For one, the cost of a supercharged increase in residency slots would be astronomical — plus, there wouldn’t be nearly enough current or projected medical school graduates to fill the spots. This mismatch between supply and demand is what has so many experts so worried about the future.
Plenty of people want to enter the medical profession, but they face training bottlenecks
It’s easy to imagine a simple solution for this problem: Incentivizing doctors from other countries to immigrate to the US. But this is not as quick a fix as it seems. Most states require doctors to complete residency training in the US, which takes at least three years. That applies even for doctors who practiced independently at expert levels in other countries; the chief of surgery at the fanciest hospital in India would still have to repeat residency in order to practice in the US.
About 13,000 of the residency match applicants this year were graduates of international medical schools, 8,000 of whom were not US citizens. But no matter how many additional doctors want to jump through the hoops necessary to practice in the US, long waits for visas and restrictive terms limiting where and for how long they can practice in the US make it unlikely many more will be added to the health care workforce in the near term. The only way to increase the number of doctors working in the US is to increase the number of doctors trained in the US.
Despite — and perhaps because of — the many challenges facing American health care, interest in entering the medical profession is high.
“There’s a genuine desire to serve,” said Green, the medical student who was facing an uncertain career future. Her story ends well: The residency match is like a convoluted game of musical chairs, with each successive round pairing still-unmatched applicants with still-open training positions. In the second round, Green found a spot in a one-year program at a hospital in Queens, New York — although for some applicants, the rounds eventually end without a job.
Finding a training program was a big personal relief for Green, but also, she hopes, a source of future relief for communities who will need her services. As a Black trainee, she sees her potential to be “an ambassador for my community as far as translating things in the health care system for them, helping them navigate the health care system,” she said. “And I think a lot of people enter the health care system with that intention.”
But not all of them can turn that intention into reality. A series of deliberate and regressive limits restrict the number of physician hopefuls who can actually get the training they need to fulfill their dreams.
The bottlenecks are by design
One major bottleneck in the physician pipeline is medical school admissions, which are only graduating about 27,000 students each year. “That started in the 1980s with the freakout over a physician surplus,” said Robert Orr, a social policy analyst at the Niskanen Center in Washington, DC. At the time, miscalculations about population growth and changes in medical care delivery contributed to a moratorium on medical school enrollment that lasted until 2005.
Although medical schools have since continued to grow, expanding too quickly could result in a surplus of medical graduates with nowhere to do their residencies. That’s because of the other major bottleneck in the pipeline — the low number of residency positions. This year’s 36,000 first-year residency slots are inadequate to meet the US need for physicians and inadequate to provide training positions for all the applicants seeking them — and like the dearth of medical school seats, it is a consequence of restrictions created long ago with arguably good intentions.
Since the Medicare and Medicaid Act was first passed in 1965, medical residents have been paid for mostly by the Medicare and Medicaid programs. The goal was to ensure Medicare beneficiaries had access to the best health care, which was thought to be found in teaching hospitals.
In 1983, Medicare made changes to the way it reimbursed hospitals for residency programs. At that time, it created formulas that calculated the dollar amount of residency training funds it supplied to each hospital as a percentage of that hospital’s care expenditures and its volume of Medicare patients — sort of like a restaurant tip, said Orr.
Those formulas have never been updated — and because they tie funding to the cost of care, they have resulted in better funding for hospitals providing high-cost care in high-cost (usually urban) areas.
Over the years, this inequitable distribution of residency program funding has meant that hospitals prioritizing primary care services in rural areas get less funding and fewer residents than those that perform lots of expensive procedures in cities. That leads to fewer primary care specialists, and because physicians often practice near where they train, fewer rural physicians.
This fee structure also incentivizes hospitals to raise the cost of the care they deliver, and results in lower funding for residency programs at hospitals that treat younger populations less likely to be covered by Medicare.
Worse yet, to reduce Medicare expenditures, the Balanced Budget Act of 1997 capped the number of resident slots that could be funded by Medicare each year. It also capped the number of residents each hospital could have at their 1996 levels, which meant hospitals couldn’t get additional residents even if the population they served ballooned in size. Obamacare undid this restriction in 2010, and since then, the number of residency spots has grown modestly.
In 2020, Congress passed a federal budget bill that provided for 1,000 new Medicare-funded residency slots to be added over the next five years. But that’s nowhere near enough to close the current gaps.
Money donated by private insurers funds some residency positions at “the hospitals with the prestige and market power to extract it,” said Orr, but “it’s not a super-equitable way of trying to get residents out to different hospitals where maybe the population isn’t as well served.”
Medical schools are growing, but residency program growth has stagnated
Since the limits on medical school seats were lifted 15 years ago, class sizes and school numbers have grown, Orlowski said. She expects the number of US medical school graduates to increase by about 3,000-4,000 over the next three years.
But still, an open question remains: Where will those graduates get residency training?
The problem of inadequate residency slots is more complicated to untangle because it requires changes in federal funding streams. While small increases in residency positions have been funded by health care institutions themselves and small investments from state governments, only a major federal investment would create the kind of growth that would end the physician shortage.
There’s not a great appetite for reform among hospitals already getting a pretty good deal under the current system, said Orr. Counterintuitively, he said, legislators from states suffering the keenest effects of the physician shortage are also less eager for change.
“Some of the biggest losers under the status quo are represented by conservative legislators, whose first gut reaction isn’t ‘Oh, we should spend more money,’” Orr said. However, he said, these legislators represent areas that are medically underserved, and have the most to gain from more residency funding. Orr favors overhauling the system to create more geographically uniform funding that is untethered from the Medicare population (and legislators’ reflexes) and encourages a more equitable distribution of trainees where care is needed most.
There are also some solutions that sidestep the residency bottleneck entirely. One of the more promising fixes to the physician shortage is to allow other highly trained providers, like nurse practitioners, physician assistants, and pharmacists, to practice independently of doctors. The American Medical Association has vigorously fought this change for more than 30 years, and physicians who oppose the move often cite patient safety concerns, although they are not substantiated by safety studies.
Much of the real motivation to prevent these providers from practicing independently may be about money and professional sovereignty; private practice doctors in particular are financially disincentivized from expanding the scope of other practitioners.
Green — who, like any good medical student, studied up on the physician shortage before I interviewed her — would like to see changes that acknowledge the breadth and urgency of the physician shortage. To her, adding only 1,000 new residency slots when the competition and need are so high just seems “a little bit absurd,” she said. “When you look at the amount of positions that we’re projected to be short, it’s a drop in a bucket of water.”
----------------------------------------
By: Keren Landman
Title: Why well-qualified medical school graduates can’t get jobs — despite doctor shortages
Sourced From: www.vox.com/22989930/residency-match-physician-doctor-shortage-pandemic-medical-school
Published Date: Fri, 25 Mar 2022 18:00:00 +0000
Did you miss our previous article...
https://consumernewsnetwork.com/politics-us/dont-leave-the-space-open-how-the-west-can-defeat-putin-in-cyberspace-and-beyond





