
LA JOLLA, Calif. — On the grounds of the University of California San Diego health system, cacti and succulents thrive where water-hogging grass once lived. Patches of bare earth await replanting or a blanket of mulch. Recycled “grey” water runs through pale purple pipes.
But the real action is inside the hospitals, where another set of pipes carry nitrous oxide. It’s a common anesthetic, also known as laughing gas, and it spews greenhouse gases that linger in the atmosphere for around 114 years. The pipes leak, a lot. Up to 80 percent of the gas can escape.
So the San Diego hospitals are planning to shut off those pipes. They’ve already done a successful pilot in the outpatient surgical center; other operating rooms are in the process of switching to storing the gas in less leak-prone tanks or canisters. Sometimes they’ll use more Earth-friendly drugs when appropriate. They’ve already stopped using another common anesthetic gas, called desflurane, which remains in the atmosphere for a decade or more, according to Shira Abeles, an infectious disease physician at UCSD, who recently became its chief medical sustainability officer.
She’s got plenty of science backing these shifts. The American Society of Anesthesiologists has identified alternatives that are better for the planet, just as safe for patients — and often cheaper.
“One hour of that volatile agent is equivalent to driving a car 250 miles, a gasoline car, I should say. And there’s very little we do in one hour,” said Joanne Donnelly, who, as director of the nurse anesthesia program at the University of Minnesota, has trained personnel in sustainable practices in hospitals across Minnesota and Wisconsin.
“Extrapolate that across an urban area, a region, a nation,” she said. “It’s an incredible impact.”

The drive to reimagine anesthesia is part of a broader if belated effort to decarbonize U.S. health care, from the operating room to the cafeteria to the gardens and grounds. It’s a push spurred on by both medical professionals and Washington policymakers, who feel increased pressure to act amid the dangers of climate change and who acknowledge health care has been slow to engage on sustainability.
The health sector is responsible for 8.5 percent of U.S. emissions of greenhouse gases including carbon dioxide, methane and ozone — an outsized impact compared to the rest of the world. (Globally, health care systems contribute roughly 4.6 percent of total greenhouse gas emissions.) Without huge new efforts, the U.S. will have trouble reaching its ambitious emissions reduction goals.
Within American health care, hospitals are the biggest source of emissions, not to mention generators of enormous amounts of nonrecyclable trash from all the single-use, disposable devices and supplies that head swiftly into landfills and incinerators.
Not every hospital is on board with transformation. Change can be expensive, and it’s always hard to overcome the inertia of the status quo. But health leaders see progress, and the Biden administration is doing its own part to push hospitals to overhaul their practices — with some success. The question is, will it be enough?
Hospitals in Vermont and Boston are growing vegetables in rooftop gardens; Seattle Children’s Hospital is planting conifers in greenery-starved poor neighborhoods. In drought-prone Los Angeles, a UCLA plastic surgeon suggested timers for operating room sinks; everyone still scrubs in, of course, but without wasting water. At the same hospital, a technician had the smart idea of setting up collection boxes for patients’ no-slip socks, a local church now launders them and distributes them to homeless people.
The sheer amount of stuff that goes to waste at hospitals is overwhelming.
Some of it is food — for patients, staff and visitors — and hospitals are increasingly shifting away from disposable plates and cups and being more consistent about reuse and recycling. Composting is more common. Some hospitals offer more plant-based meal options; New York Mayor Eric Adams, who follows a mostly vegan diet, saw to that in the city’s 11 public hospitals.
Much of it is plastic, particularly things that by design are used once and trashed. That includes many of the devices that keep a patient’s airways open, scopes used to explore inside people’s bodies, IV tubes, blood pressure cuffs, syringes. Metal items like scalpels get discarded too. Even scissors that come with a single-use label can’t be reused, even if they were only used to cut paper or gauze. Sometimes surgical instruments are tossed even if they weren’t used, simply because they were unwrapped and laid out in case they were needed.

“When you really dig into it, we find that we are typically the biggest energy user, the biggest water user and the biggest waste producer in a community,” said Barbara Hamilton, the San Diego health sustainability officer.
Sustainability leaders like Hamilton are now common at health systems; a handful have added what are known as sustainability medical officers like Abeles, physicians who connect environmental stewardship with the practice of medicine. Her background in infectious disease, for instance, can help provide assurances to her colleagues that big changes, like moving from disposable to reusable devices, are safe.
As a doctor or nurse, Abeles said, “You go with the flow and you focus on your patient care, but you’re really bothered by all the waste.
Disposable materials are convenient, but ultimately, they aren’t the only way to prevent infection. Indeed, during the early chaotic months of the Covid-19 pandemic, hospitals that used personal protective equipment that could be sterilized and reused were often in better shape than those that relied on disposables which were in short supply. But companies that form the supply chain favor single-use because it’s good for business; hospitals have to reorder the same items again and again. It’s hard to find good alternatives on the market.
Meanwhile, recycling medical waste is neither easy nor inexpensive; it’s more complicated than tossing a tuna can or yesterday’s newspaper into a blue bin. But that’s slowly changing as more health systems turn to FDA-certified companies that can recycle, sanitize or reprocess such waste. And yes, researchers have checked: Reuse is a net ecological plus, even when extra water consumption and transportation are considered.
Overall, reducing energy and swapping out the most environmentally harmful materials will — eventually — save hospitals money. Opting for reusable isolation gowns, patient transfer mats and similar goods would also leave health systems less vulnerable to shortages in the next pandemic or other emergency. Certain changes, including which anesthesia is used, can also improve patient care, noted Frances Mortimer, medical director of the U.K.’s Centre for Sustainable Healthcare, a world leader in health and climate.

But shifting to greener practices does require upfront investment, as well as cultural shifts: rethinking how, when and where all sorts of tasks are done. In numerous interviews, doctors, nurses and environmental officers made clear that change was not always easy, particularly with physicians who had been doing certain things in certain ways ever since their training.
Sustainability efforts are largely voluntary, although more of the health industry is engaging. Both new bottom-up organizations like Medical Students for a Sustainable Future as well as pillars of the medical establishment, like the accrediting body known as the Joint Commission, are undertaking the work.
One reason: It’s become harder to ignore how extreme climate events and pollution endanger human health, with poor people, minority groups and elderly people particularly vulnerable. Extreme weather exacerbates heart, lung and kidney disease; it makes asthma worse. Mental health deteriorates. Heat waves kill people — directly, or by aggravating chronic conditions. Power outages in patient homes mean no refrigeration for insulin or electricity to keep oxygen tanks flowing.
Indeed, many hospitals are making a related, but distinct, effort to become more resilient to the fallout from climate change. Resiliency enables hospitals to withstand the impact of worsening hurricanes, floods, wildfires or heat domes. Decarbonization and efforts to bolster sustainability aim at combatting climate change itself.
“What excites me is that health professionals are starting to connect the reason why they’re there in the first place, which is to take care of patients, with the health impacts that are happening because of climate [which] their health systems are contributing to,” said Shanda Demorest, a nurse who is associate director for climate engagement and education at Health Care Without Harm, which along with its Practice Greenhealth arm, is a major force in pushing for new health and climate work.
Early in the Biden administration, officials took some real steps, both practical and symbolic, to make combatting climate change a greater focus in American health care.
The Department of Health and Human Services signaled the issue was a new, formal priority through the creation of the Office of Climate Change and Health Equity, though it’s running on a patchwork of staff borrowed from other offices and agencies since Congress hasn’t funded it. In May of last year, HHS Secretary Xavier Becerra added the Office of Environmental Justice to address the disproportionate harm pollution and climate change inflict on low-income and minority communities.
The Veterans Administration and the Indian Health Service, which deliver health care to millions of people across the country, have been directed to reduce emissions and energy use as part of the Biden White House’s overall government climate policy.
For the rest of the health care system, HHS unveiled a Climate Pledge on Earth Day 2022 to spur more action. It was originally a one-time opportunity to create a vanguard for change. But hearing that more organizations were ready to come on board, HHS recently decided more hospitals can sign on, with public lists being updated twice a year — coinciding with the U.N. International Climate Conference in the fall, and Earth Day in the spring. About 116 health organizations, representing 872 hospitals as well as other health care sectors, have signed on. Along with the federal health systems, that represents about 15 percent of U.S. hospitals, HHS officials said.

The climate pledge is voluntary, but hospital sustainability experts insist it’s not the usual feel-good exercise. Signatories commit to specific actions and must publicly report progress toward cutting emissions by 50 percent by 2030 and cutting net emissions by 100 percent by 2050.
“It’s been a catalyst,” said Sarah Brockhaus, the sustainability programs manager of UCLA Health, sipping from a recyclable cup in a hospital cafeteria. “It’s a public pledge … we will be held accountable.” There’s also a trickle-down effect in terms of knowledge and experience, she said, for smaller hospitals and those with fewer resources than a place like UCLA. “The work we are doing will be shared.”
Joe McCannon, a senior adviser to the HHS climate office, said that one reason for the pledge was “to show that organizations can really move the mark on both resilience and on decarbonization.” Another reason, he said, was to “create a community … to bring together like-minded organizations to learn from each other to become exemplars and create some shared accountability.”
If enough hospitals join up, they can also throw their weight around. This “community” could develop enough purchasing clout to change the market, to force it away from all those disposable goods. HHS has also discussed aligning procurement standards with the U.K.’s National Health Service, which could bring about faster market changes and perhaps encourage other countries to do the same.
HHS has rolled out resources — webinars, toolkits, technical advice — that are available to all health systems. The climate provisions in the Inflation Reduction Act also provide tax breaks (or similar financial incentives for nonprofit health systems) for improving energy efficiency, moving to renewables and reducing harmful air pollution. Generally, there’s more activity in Democratic-led states.
Going green is also easier for big, relatively resource-rich systems like the multi-campus University of California Health — though not all academic medical centers are equally engaged. Some small community hospitals, big for-profit chains and safety net hospitals are also reducing their carbon footprint. But it’s harder for hospitals with fewer resources, even though their communities are hardest hit by climate and pollution, said Kalpana Ramiah, vice president of Innovation at America’s Essential Hospitals, the safety net trade group.
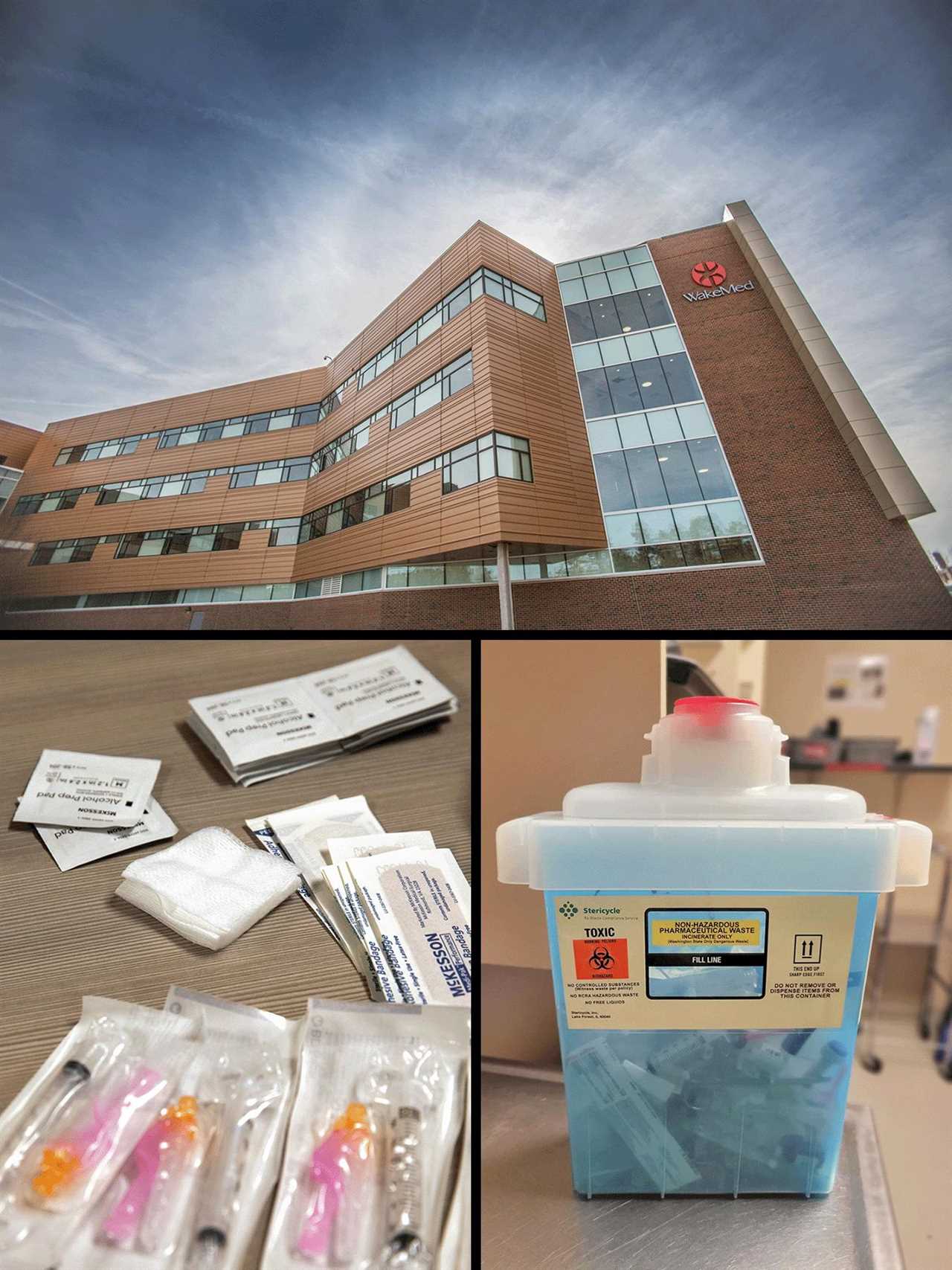
WakeMed, a hospital that provides 90 percent of indigent care in the Raleigh, N.C., area, started addressing energy efficiency a decade ago — replacing HVAC in its old buildings, building greener designs in its new ones. There’s a garden and egg-laying hens near one campus; Tom Cavender, the hospital’s vice president for facilities and construction said touting “farm to table” food helps in a market dominated by massive health systems run by Duke and the University of North Carolina.
The hospital wasn’t ready to sign the original HHS pledge; a spokesperson said it’s now aiming for late 2023. Meeting the standards won’t be easy. “The zeal and the zest to do it is there,” Cavender said. “It’s the financial obligations that it takes to get there.”
Resource-intensive health care has all sorts of other unique challenges. It’s pretty easy for people to switch to LED lightbulbs or start transitioning to electric vehicles. But MRIs gobble up huge amounts of electricity and the machines can’t be turned off completely. Hospitals are now working on energy-smart scheduling and utilization, including times when they can be on low-power.
A big facility like the Ronald Reagan UCLA Medical Center can’t just shut off all of its operating suites at night and on weekends; it’s a trauma center and a transplant center, and it needs 24/7 readiness. But that doesn’t mean every operating room has to be fully fired up every minute, said Arturo Sanchez, the administrative director of sustainability. UCLA Health is now studying things like “HVAC setbacks” and “equipment shutdown protocols” and learning how other hospitals have powered down some of their operating rooms without sacrificing preparedness.
Little changes make a big difference when they go to scale.
For instance, Providence, a large Catholic health system aiming for net carbon neutrality by 2030, used to have disposable plastic boxes for collecting “sharps” like needles and scalpels “in every patient room and a lot of other places,” said Beth Schenk, a nurse who is executive director of Providence’s Environmental stewardship. They’ve been replaced with new containers that can be used 600 times; in a system with more than 50 hospitals and 950 clinics from Alaska to Texas, it’s a big change.
Progress is uneven; clinicians or staff can be set in their ways, although Health Care without Harm’s Demorest and others reported that as their communities see the consequences of climate change firsthand, the pull of stewardship becomes stronger. They don’t just become more open to change; they instigate it.
For instance, it’s hard to recycle trash once blood gets on it. So, nursing students at UCLA came up with the idea of removing packaging and prep materials from the operating room before a patient is wheeled in, said Chris Clevenger, a nurse who oversees the main operating room.
All this adds up to a lot of activity — but not enough to decarbonize the health sector as quickly and deeply as needed.
Chisara Ehiemere, a leading researcher at NYU Stern Center on Sustainable Business, is gathering data on the health sector and climate. The early adopters, she said, are on their way. But health systems that didn’t start sustainability efforts before the pandemic probably didn’t start during the pandemic, and now “their hands are full” with managing the Covid fallout, from nursing shortages to slim margins. For them, unless and until the data shows clear return on investment for green initiatives, “It’s really hard sometimes for hospitals to make the business case for doing this.”
On the other hand, she said, if hospital leaders start to perceive climate action as unavoidable — either because they anticipate it will be mandated or because they will face mounting pressure from within, particularly from younger doctors and nurses — they may start sooner rather than later.
HHS is aware that not all health systems are committed, and that even those that are may need help. McCannon said HHS is rolling out technical assistance and some grants.
But activists and sustainability teams want more. More tools. More metrics. More financial help.
Some advocates would like to see the federal government impose tough regulations and requirements to force change. Others suggest building incentives into Medicare payments to hospitals, which would give a government-imprimatur on health care greening without creating a new mandate. Climate benchmarks could be included in HHS’ “conditions for participation,” the practices that health providers must follow to be eligible for Medicare or Medicaid payments.
Any such steps, though, would be challenging in today’s political climate, with Republicans strongly opposed to efforts to the Biden administration’s efforts to tackle climate change.
Still, it’s clear that sustainability work is gaining momentum in health systems of all kinds across the country.
“I do think there’s a domino effect,” said the University of Minnesota’s Donnelly. “People have accepted that there is a great challenge, and that they want to be part of the solution. They want to join. They just need to know how.”
----------------------------------------
By: Joanne Kenen
Title: Turn Off the Laughing Gas
Sourced From: www.politico.com/news/magazine/2023/06/06/hospital-climate-change-waste-00098612
Published Date: Tue, 06 Jun 2023 03:30:00 EST





