

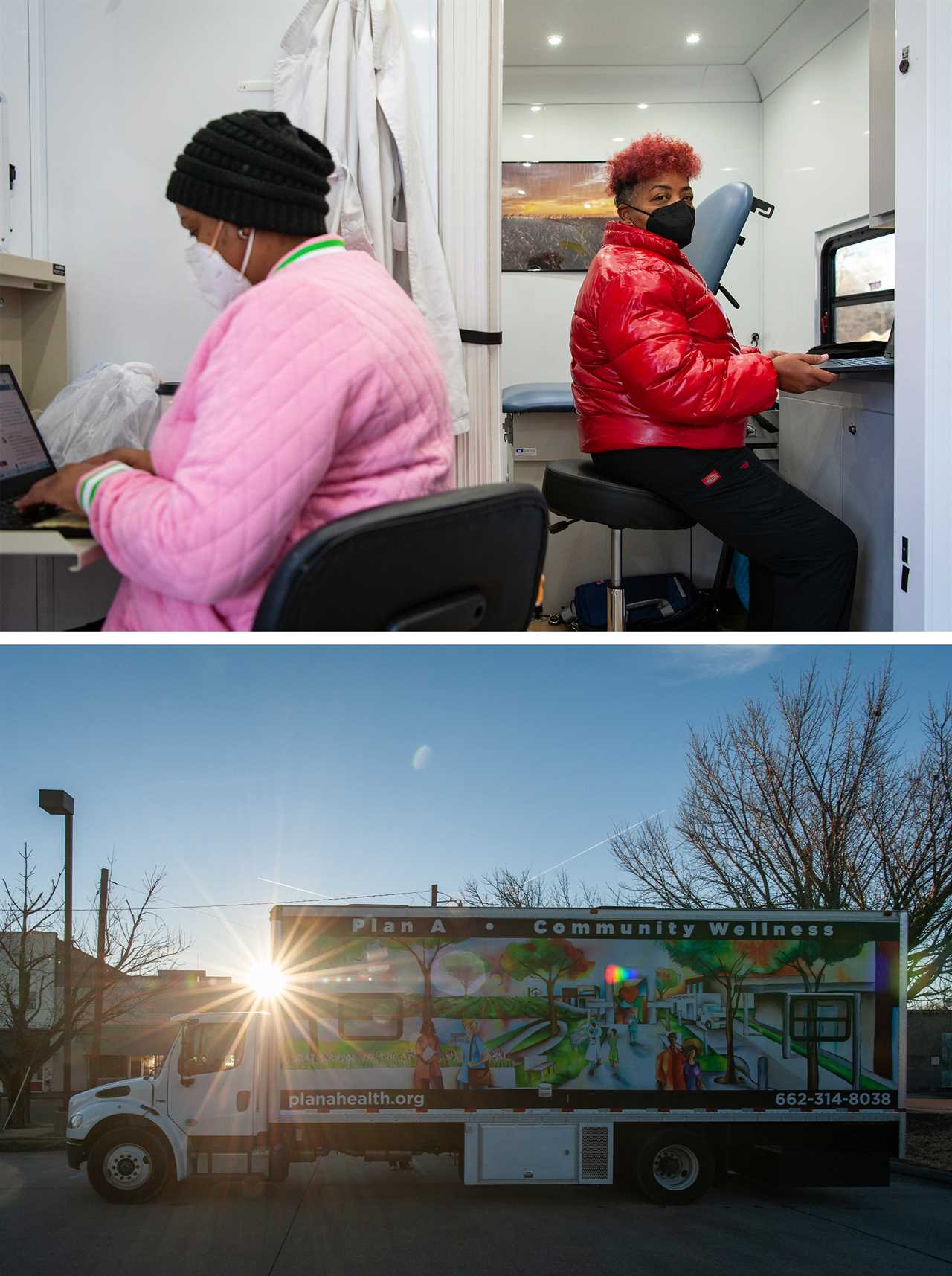
INDIANOLA, Miss. — On a humid day in late September, a box truck with images of people and trees decorating the cargo trailer was parked in front of a home goods store in this small town. Juliet Thomas, a community health worker, stood at the foot of the steps that descended from the trailer. Thomas is in her early 50s, with short hair that was platinum on top, and she had her eyes trained on a young woman who was perusing a table arrayed with modest schwag: a stress ball shaped like the truck, educational pamphlets about Medicaid, blue rubber bracelets. The woman reached out and touched a bundle of condoms, then pulled her hand back.
“Go ahead now,” Thomas said, her face lit by good humor. “You need ’em, you need ’em.” The young woman started laughing, grabbed the condoms and let Thomas lead her into the trailer.
Inside was a 260-square-foot space with two exam rooms, a bathroom and even a small lab space — the mobile health care clinic run by Plan A Health, a nonprofit that provides free reproductive, sexual and primary care in towns across the Mississippi Delta. Thomas and her colleagues spend their work week traversing the Delta’s highways, usually visiting a single small community in a day and, by doing so, testing out a new, portable model for improving reproductive care in rural America. Once a patient enters Plan A’s clinic, either Thomas or a colleague does a blood pressure and blood sugar test, and then gently broaches the clinic’s other services. Does the patient want to discuss family planning? Would she like an HIV test? Does she need a test or treatment for a sexually transmitted infection?

Thomas, who grew up about 30 minutes away in Greenville, Miss., formerly worked as a field representative for Rep. Bennie Thompson (D-Miss.), and she knows how deep-rooted her patients’ challenges are. The history of slavery, sharecropping and segregation shadows life in the Delta, the stretch of the state that borders the Mississippi River and runs roughly between Vicksburg and the Tennessee border. It’s where the civil rights activist Fannie Lou Hamer was born and where 14-year-old Emmett Till was lynched in 1955, after it was said he whistled at a white woman outside Bryant’s Grocery — the ruins of which lay a short drive from where Plan A was parked. Today, half of Delta counties are more than 70 percent Black. Most have poverty rates between 25 and 45 percent, compared with the national rate of 12 percent. Health outcomes here are dismal. Over the past 40 years, mortality rates have fallen across the country, but they’ve increased in the Delta.
Plan A’s focus on reproductive and sexual health means most of its patients are women. And although Plan A doesn’t provide abortions, it does offer pregnancy tests and helps patients move forward with any decision they make after learning the results. So, the clinic’s staff, including founder and executive director Caroline Weinberg, knew they were entering politically fraught territory when they began offering services last April. In December, the U.S. Supreme Court heard arguments in Dobbs v. Jackson Women’s Health Organization, the case involving a 2018 Mississippi law that would ban abortions after 15 weeks of gestation. That ruling, expected later this year, is likely to upend Roe v. Wade, the landmark 1973 case that gave Americans the right to seek an abortion, as well as Planned Parenthood v. Casey, the 1992 case that affirmed abortion access as a constitutional right.

A brief filed by Mississippi Attorney General Lynn Fitch summarized the state’s arguments, writing that Roe and Casey are wrong and outdated, in part because contraception is accessible, affordable and effective, and because today “on a wide scale women gain both professional success and a rich family life.” This argument has been echoed by other proponents of restrictive abortion policies. But what Thomas and her colleagues have seen first-hand in roughly a year of operating their clinic is that many Mississippians do not enjoy easy access to contraception — let alone other basic medical services necessary to plan families and thrive.
Rates of babies who are born underweight, for instance, are very high in the Delta. That’s obviously bad for babies, but it’s also considered a key indicator of the health of mothers, revealing that women in the region experience high levels of stress and poor access to health care. Plus, the state, like many rural areas, has an obstetrician-gynecologist shortage. In more than half of Delta counties, there’s not a single OB-GYN, according to federal data. Plan A has had an insured patient contact them for help getting an IUD, because she couldn’t find an appointment elsewhere for less than three months in the future.
The majority of patients who visit Plan A are uninsured or underinsured, struggling both to afford health care and to physically access it in a sparsely populated region where the nearest hospital or doctor might be an hour’s drive away. Even a health care provider situated a half-hour away can be unreachable without reliable public transit, and telehealth has limitations in the Delta, where many lack broadband access. Patients also might hesitate to seek out care — especially for a sexual health issue — because they feel alienated and judged by a medical system that doesn’t always treat the poor or people of color with dignity. Some rural health providers don’t offer family planning or gynecological exams at all. Meanwhile, the Covid-19 pandemic has pushed many of the state’s beleaguered health care workers out of the industry altogether.
To some extent, Weinberg, who went into public health after completing medical school, anticipated these problems, and figured that a mobile clinic could help address the core issue of geographic isolation. She hoped that making services free, as well as staffing the clinic with people who lived in the Delta and looked like their patients, would build the trust needed to deliver care around sensitive issues such as HIV, STIs and birth control. But, over time, the regional challenges she learned about before the clinic ever saw a single patient have revealed themselves to be much deeper, prompting the organization to expand its services beyond reproductive and sexual health to become a broad-based provider, addressing basic needs such as primary care and vaccinations. It was only Plan A’s second day, for example, when the staff encountered its first medical emergency. The clinic had arrived at a factory in Greenville to offer employees free health screenings when a seemingly healthy woman walked into the truck; she had a blood pressure of 220 over 110 — a life-threatening level. Since then, it’s been a rare week when Plan A doesn’t see someone with blood pressure high enough to warrant a visit to the emergency room.
So far, Plan A’s mobile staff of three — Thomas, nurse practitioner Toria Shaw and another community health worker named Antoinette Roby — has traveled more than 600 miles, visited more than 30 towns and seen about 600 patients. More than half of their patients have received sexual and reproductive health services. Plan A also has given out nearly 200 Covid-19 vaccines.
What’s worked for Plan A over the past year has been cultural sensitivity and individualized care, as well as near-constant assessment of how they can better serve clients and an acute awareness of potential pitfalls. Weinberg knew that, as a highly educated white New Yorker, she was “an outsider on every level,” in her words, when she conceived of Plan A, and so she tried to network with anyone who would answer their phone in the Delta — elected officials, health care activists, clergy, nonprofit leaders — to get feedback on her vision, as well as their advice for building trust. “It’s not fair to come into the community and not find out how they feel,” says Jackie Sanders Hawkins, a veteran health outreach worker from the Delta who eventually joined Plan A’s board. “She was able to touch base with all those different stakeholders. Had she not done that in the beginning, then the clinic probably would not have been here.”
Inside the truck, Thomas and her colleagues go out of the way to make patients feel comfortable and do persistently follow up to make sure patients pick up their prescriptions or make it to specialist appointments. Patients, in turn, have told Thomas and her colleagues about a variety of issues that affect their health: relationship problems, infertility worries, sexual abuse and the lingering grief of miscarriage. Many have confided about suffering from chronic pain and heavy bleeding caused by uterine fibroids. Others have talked about relying on tissues to absorb menstrual fluids because tampons and sanitary pads are too expensive. “Some people we touch,” Thomas says. “And they open up to us about certain things in their lives.”
Plan A’s approach has the potential to be replicated, and the organization is working to expand. But its work also underscores the depth of patient need, and demonstrates just how hard it is to serve rural patients well and how many more resources are needed to address race-based and geographic health inequities in a more comprehensive way.
Health and race are inextricably linked in Mississippi. Black and Native American residents, for instance, are far likelier than their white neighbors to die early from treatable conditions. Black women in Mississippi die of cervical cancer at a rate nearly twice the national average. Pregnancy-related deaths for Black Mississippians are nearly three times the rates for white women. Black babies, too, die at nearly twice the rate of white infants in the state.
The state is arguably the most extreme case of the much-discussed national crisis in rural health care, in which policy, geography and demographics translate into bankrupt hospitals, provider shortages and pharmacy deserts. Covid-19, and the speed at which it spread through rural America, shone a bright light on the disparities between urban and rural health systems. Mississippi, whose health system the Commonwealth Fund foundation ranks as the poorest performing in the country, has seen five hospitals close between 2010 and 2019. An additional 27 are classified as vulnerable, according to the National Rural Health Association, a nonprofit membership organization. Mississippi also ranks dead-last among states in physician-to-population ratio.

These problems are exacerbated by the fact that Mississippi is one of 12 states that have declined to expand Medicaid under the Affordable Care Act, a critical source of revenue for hospitals and a safety net for poor Americans. Tim Moore, president and CEO of the Mississippi Hospital Association, a statewide trade organization, says Mississippi’s rural hospitals frequently see patients with conditions that might have been prevented with regular access to a doctor. Those are the people, Moore says, who end up disabled and dependent on Supplemental Security Income, a cost to the state that he says could be prevented by insuring more Mississippians.
Last year, Moore’s organization pushed to get Medicaid expansion decided by ballot initiative, but the effort was upended when the state supreme court invalidated the initiative process in a separate case. In September, Mississippi state economist J. Corey Miller, the director of a public research center that works closely with state government, concluded that expanding Medicaid would provide coverage to an additional 228,000 to 233,000 Mississippians, and also boost state revenues, GDP, population and jobs. Ninety percent of the costs associated with expanding enrollment to those people would be covered by the federal government, which also has offered holdout states a temporary increase in Medicaid matching funds. Miller estimated that the latter could save Mississippi more than $600 million in 2022 and 2023.
Lt. Gov. Delbert Hosemann, a Republican, has recently hinted to state media outlets that he supports Medicaid expansion. But House Speaker Philip Gunn and Gov. Tate Reeves, also Republicans, have publicly opposed it. “My position has not changed,” Reeves said last year. “I am opposed to Obamacare expansion. This was a major issue in the governor’s race, in both the Republican primary and the general election, and the people have spoken on that issue.”
According to the American College of Obstetricians and Gynecologists, policies that decrease Medicaid access and services disproportionately hurt women, in part because the program is the largest payer of pregnancy services, and also because women with Medicaid get more preventive care than the uninsured, which results in fewer breast cancer deaths and adverse fetal and maternal outcomes. Medicaid also is critical for low-income people seeking contraception, accounting for 75 percent of public expenditures for family planning services in 2015, according to the Guttmacher Institute, a research organization that supports abortion rights.
Another key source of publicly supported contraceptive access are clinics supported by funds through Title X, a federal program established to provide family-planning care to low-income people. In Mississippi, the grantee for Title X funds is the state department of health, and the vast majority of Title X clinics are the state’s county health departments. But the closest health department can be hard for people in the Delta to access; some offices are open only once or twice a week, or only offer family planning services once a month. A spokesperson for the Mississippi State Department of Health said in an email that the state, like the rest of the nation, suffers from a shortage of providers, and that the department of health is not the only source of reproductive health available for free and for low-income women.
Kari White, director of the Mississippi Reproductive Health Access Project at the University of Texas at Austin, says that, when she started doing research on contraception access in the state in 2016, she was struck by “just how inaccessible the public health department services were.” People she interviewed reported waits of a month to get services. A brief White co-authored found that Mississippians seeking contraception at a health departments and other providers frequently faced limited choices of contraceptive methods, appointment delays of four weeks or more, and sometimes requirements to make multiple appointments at different locations.
“If you have to drive an hour to get your birth control, who has to take you?” asks Laurie Bertram Roberts, co-founder of the Mississippi Reproductive Freedom Fund and executive director of the Yellowhammer Fund, two organizations that assist people seeking abortions in the Deep South. “Is it your abusive partner who may or may not want you to have it? There are logistical hurdles.” Timely access to birth control is obviously important to anyone trying to prevent pregnancy, but sexual and reproductive care also can be the only touchpoint with the medical system for society’s poorest and most marginalized — the only place to detect health issues that can profoundly affect patients and their families. “I know people who have terminated pregnancies that they wanted to carry to term,” Roberts says, “but they have conditions that have not been managed.”
In early December, the Plan A truck sat beside the bell tower of Turner Chapel AME Church, a historically Black congregation situated in a neighborhood of Greenwood, Mississippi, that’s characterized by cottages with security doors and wide, shaded front porches. The Plan A truck is tight, with scant space to squeeze between its exam tables and fold-out work desks. Thomas, Roby and Shaw spend a lot of time crammed inside together. Even on non-travel days, they are in frequent communication: juggling patient follow-ups and paperwork, identifying places for the clinic to visit, and establishing or reinforcing relationships within communities. One weekend, Thomas didn’t call Roby at home, and Roby’s husband expressed concern. “I said, ‘Well, we ain’t working,’” Roby recalled. “And he said, ‘Nah, y’all relationship more than work.’”
An outgoing woman who used to drive big rigs, Roby was hired to drive the Plan A truck but has transitioned into a community health worker role, too. She gestured at her backpack, which was stocked, as usual, like its own miniature clinic: gloves, masks, clipboard, pens, glucose meter, condoms, specimen containers and a secure pouch to keep patient records private. “I’m picky, I’m picky,” Roby said. “I got, like, five or six notebooks to put all our information and stuff in — you know, everything that we have to do. I’m precise with everything.” She’s similarly attentive with the people who visit the clinic. One of the patients that day was Willie Magic, an uninsured 53-year-old with a rail-thin body who had lost his job at a catfish farm after a seizure sent him tumbling down a flight of stairs. He had come for a Covid-19 booster shot because “people are dying,” he said.
Magic wasn’t necessarily the client Weinberg imagined when she initially imagined a free clinic for reproductive and sexual health, but Plan A adjusted its offerings in response to focus groups the organization led across the Delta with locals and community leaders — resulting in a range of new or modified services over time. Early on, a few focus group attendees, for example, told Weinberg that Delta communities desperately needed routine primary care in whatever form and at whatever frequency it could be delivered. So, from its inception, the truck has seen adult patients of any age and gender, as well as adolescents; they now discuss diabetes management and heart health regularly.
The range of services also provides a shield for people in the Delta who are worried about privacy in small towns: Patients might not want to walk into a clinic their neighbors exclusively associate with HIV testing and birth control. That’s part of why Weinberg’s hires come from bigger Delta towns — Roby and Thomas from Greenville, and Shaw from Batesville — rather than from somewhere tiny, such as Alligator or Rosedale. Adolescents in particular expressed intense privacy and transportation concerns, spurring Plan A to work with after-school programs that serve youth to offer STD testing and treatment, as well as birth control.
By December, Plan A had learned other lessons, too. Weinberg hadn’t anticipated, for instance, that the clinic would be talking so frequently about fertility, but patients kept showing up with questions. Shaw usually offered advice on the normal timelines for conception and, if a patient had been trying unsuccessfully to conceive for over a year, blood tests. Abnormal bleeding was a common complaint, so the clinic got a machine that facilitates spot checks for anemia, which can be an indicator of uterine fibroids, a condition more likely to affect Black patients than white.

In Greenwood, during a lull between patients, Roby and Thomas stood outside the truck, soaking up the winter sun and recalling the demand for another service, Covid-19 vaccines, that emerged in late summer and fall, as the Delta variant surged in the state and news outlets began publishing photographs of overflowing hospitals erecting field units in parking garages. “We kept letting Caroline know,” Roby said. “You know, ‘We was here in this town, and a couple of people came up to the unit and asked if we gave out Covid shots.’”
Thomas, who had switched her hair color from blonde to bright red by this point, chimed in. “We don’t like saying ‘No,’” she said. “We don’t like that.”
So, now Plan A was hosting vaccine-centered days like this one, which had been arranged at the request of the church’s pastor, Rev. Alice H. Crenshaw. “The need is great,” Crenshaw told me. She spent part of the day on foot around town, trying to persuade people to visit the Plan A truck. She stopped to chat with a woman gardening, with a couple outside a gas station and with a group of people who were drinking beer beneath the trees outside a corner bar.
Anyone who accepted her offer found Rohith Reddy, a second-year medical resident from Delta Regional Medical Center, a Greenville, Mississippi, hospital, inside the clinic, where he had spent most of the morning asking patients to roll up their sleeves for a quick jab. Reddy’s time with Plan A, part of a community health rotation, was one of several experiences in the Delta that made him want to remain in the state after his residency. “People actually need health care here,” he says. “It’s not a choice. I want to stay here, to do my part for five years, 10 years.”
Even as Plan A’s offerings have expanded, women’s health remains at the core of its mission. For Reggan Mason, who visited the Plan A truck in October, when it came through Clarksdale, being able to get a Pap smear at Plan A and get help accessing a free mammogram through a cancer screening program run by the Mississippi State Department of Health offered peace of mind. “It was wonderful,” she said. Her sister died of breast cancer in 2016, and she knew the dangers of skipping screenings. “I felt like I was back on schedule.” Mason works as a clerk in a medical office but doesn’t have health insurance because she is classified as an independent contractor.
Women like Mason are what drew Shaw, Plan A’s nurse practitioner, to the organization. Shaw, who has 22 years of experience in health care, liked that Plan A would be totally free, with no cost to see a provider and no surprise bills for lab tests. She had worked in other clinics with income-based sliding scales for fees and seen how even a $100 bill could be devastating for someone supporting her family with a job in a gas station or a cafeteria. She often remembers a woman she met on a cancer ward in Tennessee: a 32-year-old single mother with cervical cancer that had metastasized, an outcome that could have been prevented with routine Pap smears.
“The communities that we serve — women are the backbone of their families,” Shaw says. “And usually they do forego their care to take care of everybody else in the family. Now that’s historic, and in many, many cultures, but especially in the African American community.”
Plan A’s broad interest in reproductive justice places it in a potentially delicate position in a conservative state. Thomas and Roby are often careful to talk about “family planning” rather than “birth control” with clergy, for instance. But so far, local officials and community leaders in the Delta — a blue region in an otherwise red state — have met Plan A with support. Ruffin Smith, the mayor of Louise, a town of 200 people, put it this way: “I don’t know why anyone would not want an organization offering medical services where there were none.” In October, Thomas Dobbs, the state health officer, posted on Twitter about Plan A, calling it “a phenomenal community resource” and including a photograph of himself standing with Roby, Weinberg and Thomas.

Weinberg says she built the organization under the assumption that Roe v. Wade would be overturned, and that policies around reproductive rights would only get more restrictive. “We worked to make sure we could do what we do within the bounds of America right now,” she says. “The [Dobbs] case, if it goes through, for us, functionally, it doesn’t change anything. We’re not offering abortions in the clinic.” But, she says, “It has an extraordinary impact on the people we serve,” meaning any pregnant person they refer for care could soon find their options far more limited.
While Plan A might bill Medicaid someday, it’s designed to stay solvent without doing so. The nonprofit covers its costs with in-kind donations; foundation, corporate and individual donations; and government grants. It has a full year’s worth of organizational expenses, which run around $600,000, either banked or committed. Plan A is also exploring how its model might best be adapted to communities in other parts of America. It’s currently evaluating its clinic, alongside three mobile health clinics in other states, to assess how well the mobile concept works for increasing reproductive and sexual health care access.
If some of Plan A’s approaches prove scalable, it wouldn’t be the first time the Delta served as a proving ground for innovative ideas. In the 1930s, women from Alpha Kappa Alpha — the historically Black sorority that today counts Vice President Kamala Harris as a member — organized the Mississippi Health Project to bring mobile medical services, including testing for sexually transmitted diseases, to impoverished Delta sharecroppers. The project immunized more than 15,000 children against diphtheria and smallpox, and treated thousands of adults for other various issues. It ended in 1942. The nation’s first rural community health center also was established in the Delta, in the town of Mound Bayou in 1967, by doctors who included civil rights activists Count D. Gibson and H. Jack Geiger. Their Mound Bayou clinic eventually inspired the development of nearly 1,400 health centers that are visited every year by more than 30 million Americans across the country. Still, health centers like these faced shrinking revenues during the pandemic and are also challenged by workforce shortages and rising medical costs.
Weinberg shares some of Gibson and Geiger’s idealism and ambition, acknowledging the ways that social factors — such as access to jobs, education, race and safe housing — intersect with health, and noting that Plan A’s ultimate dream is for everyone to have access to the reproductive and sexual health care services they need to live the future they want. “But also, we’re not in a position to take on the world, so we focus on the communities we focus on,” she says.
Systemic change would likely require the attention of state and federal policymakers. Carrie Cochran-McClain, the chief policy officer at the National Rural Health Association, says rural patients would benefit from extending the reduced restrictions around telehealth that Congress implemented during the pandemic. The CDC could establish an office of rural health as a focal point for grants and research, she adds. In Mississippi, as in many other states, some policies also complicate efforts to provide convenient care to low-income and rural people. Plan A, for example, has abundant supplies of birth control pills, Weinberg says, but discovered a rule, designed to minimize potentially dangerous interactions between different drugs, that prevents the clinic’s nurse practitioner from handing medication directly to patients; she has to write a prescription and send patients to the pharmacy — one more step, one more chance for people to slip through the cracks.
Rural health and health equity advocates expressed some optimism about reforms in the Biden administration’s Build Back Better legislation. The bill would have reduced the gaps in Medicaid coverage that affect children and pregnant people, who can lose coverage 60 days after giving birth, for example. (The state Senate in Mississippi recently passed a bill to extend this coverage, but it died in the House.) Build Back Better also offered a workaround so people in non-Medicaid expansion states who fall within the coverage gap could access and afford the ACA marketplace. But with the legislation indefinitely stalled, dwindling networks of rural for-profit and nonprofit health care providers are still trying to fill these gaps, and stay afloat while doing so.

Louise, Mississippi, was sleepy on a cloudy morning 10 days before Christmas. Little was open in the four-block downtown other than city hall and the post office, both of which face a row of silvery grain silos. Plan A’s mobile unit was parked and locked, and Roby, Thomas and Shaw were instead working inside one of the storefronts. That brick-and-mortar clinic was one more thing that Weinberg had zero intention of running when she began working on Plan A, but Smith, the mayor, had offered them the space, and now the organization works from a regular building twice a month.
Patients had arrived as soon as the doors opened at 10 a.m., and the waiting room was jammed with young women and older adults, the latter of whom were mostly waiting for booster shots as Omicron had begun dominating headlines. Roby sat in the reception area behind a black laptop, her trusty backpack within arm’s reach, alternating between entering patient records into the computer and texting questions to Weinberg, who was at home in New York.
Thomas worked at an adjacent desk with a sparkly reindeer headband atop her red curls and a bag of holiday decorations she had bought at her feet. She was on the phone, trying to ensure that a medical exam Shaw was about to administer to a patient would satisfy an insurer’s application requirements for enrollment. “What all needs to be covered?” Thomas asked. “I don’t want to do a medical exam that disqualifies him from anything, that leaves anything out. I don’t want to delay this process.”
Thomas and Roby spend a lot of time on the phone. Shaw writes the prescriptions, but it is usually Roby or Thomas who call patients to make sure those prescriptions get filled and taken. If Plan A schedules a free mammogram for a patient, Roby or Thomas call to make sure they remember to go, and that they have transportation to get there. They assist patients in navigating the red tape to apply for Medicaid or other insurance, and they address problems that aren’t explicitly medical, such as helping a patient find safe and secure housing; as many clinics do, Plan A also makes voter registration forms available. Roby sometimes gives out her personal phone number, and some patients call just to talk.
These calls sometimes reveal the limitations of what Plan A is doing. The team called one patient and heard she had gone to a pharmacy only to encounter an $800 bill, so Plan A decided to build a free pharmacy, which opened in the Louise clinic in November. They also realized that some women hesitate to get Pap smears — even free ones — because they’re terrified they’ll receive an abnormal result and be unable to afford treatment; the organization has tried to ease these anxieties by adding equipment to do colposcopies, which are diagnostic, and LEEP procedures, which remove abnormal cells from the cervix.

The demand for prenatal services has been intense as well, and Weinberg is trying to find ways to offer more comprehensive prenatal care. Down the line, Weinberg would like to serve transgender patients who are transitioning. And she’s actively working on making the Louise space available to other providers — cardiovascular specialists, dentists, social workers — who might want to bring additional free services to the community.
But everything represents a risk. Do too much, and the program could collapse on itself; spend too freely, and there’s less money to pay for patients’ lab work, one of the clinic’s biggest costs. This year, Plan A wants to serve 2,000 people, but there are a lot of variables, including Covid, which has put a halt on communitywide health fairs where they might, for example, be able to do HIV and STD tests for 50 people in a single day. Just last week, the organization finished raising the funds to buy a second truck, which they hope to deploy in another, yet-to-be-determined state with similar health challenges: restrictive policies around reproductive care, large uninsured populations, and high rates of unintended pregnancies and STDs.
Weinberg and her team also know they’re only as good as the reputation they build in the Delta. “When we first started out, I was expecting that people were going to just run to the free services,” Roby says. “No, they don’t. It’s the trust. It’s getting them to trust new people.” She says she’s hyper-aware of her words and careful to avoid sending out any “bad vibes,” even unintentionally.
In Louise, shortly before noon, a patient scheduled a follow-up appointment, then leaned over the window into the reception area and good-naturedly pointed an index finger at Roby “Don’t call me, don’t text me, nothing,” she said. Roby laughed and looked her in the eye, “You know I’m going to, though.”
For the moment, though, neither Roby nor Thomas nor Shaw could think about the patients they would see or call tomorrow. They were so busy that Roby’s breakfast sandwich sat half-eaten in a Styrofoam container on her desk. Shaw was mentoring an earnest new resident, while also juggling a variety of cases: a woman who took a gonorrhea test and wanted to discuss birth control, another person fretting about the price of insulin, older patients who needed Covid-19 and flu shots. A young woman with luminous skin and an infant on her shoulder followed Thomas down a hallway to an exam room.
Thomas returned a few moments later and dropped paperwork in a plastic tray. Her shopping bag of golden tinsel and felt stockings had been stashed on a shelf and forgotten. No one had time to decorate yet. Too many people were waiting.
----------------------------------------
By: Vanessa Gregory
Title: How Three Women in a Truck Are Trying to Fix Rural Mississippi’s Health Woes
Sourced From: www.politico.com/news/magazine/2022/03/18/mississippi-delta-plan-a-mobile-health-clinic-00007251
Published Date: Fri, 18 Mar 2022 03:30:00 EST





